Primary penile melanoma is an aggressive and rare neoplasm (less than 1.4% of primary penile cancers) that affects patients in the sixth and seventh decade of life.[ 1 2 ] The first case was described by Muchison, in 1859.[ 3 ] Histologically, it is classified as cutaneous or mucous (most frequent). The cutaneous melanoma compromises 9% of the cases and it is located on the penile shaft. The mucous melanoma is located mainly in the glans (55%), foreskin (28%), and urethral meatus (8%).[ 1 4 ] The curative treatment is related to the excision of the tumor in its initial growth phase, so the requirement for an early diagnosis of these lesions is well established.
A 66-year-old Caucasian, male, non-smoker, from the city of São Paulo, attended the urology department due to an injury to the penile glans of insidious growth for 1 year. There were no other associated symptoms. On physical examination, he had a 1cm, ulcerated, painless, hyperpigmented penile lesion surrounded by satellite lesions. There were no palpable perilesional lymph nodes or inguinal region (Figure 1).
Figure 1 A. Ulcerated lesion with erythematous and blackish-brown areas of irregular shape, surrounded by erythematous and brownish papules on the left side of the penis glans; B. Satellite lesion on the dorsal surface of the penis.
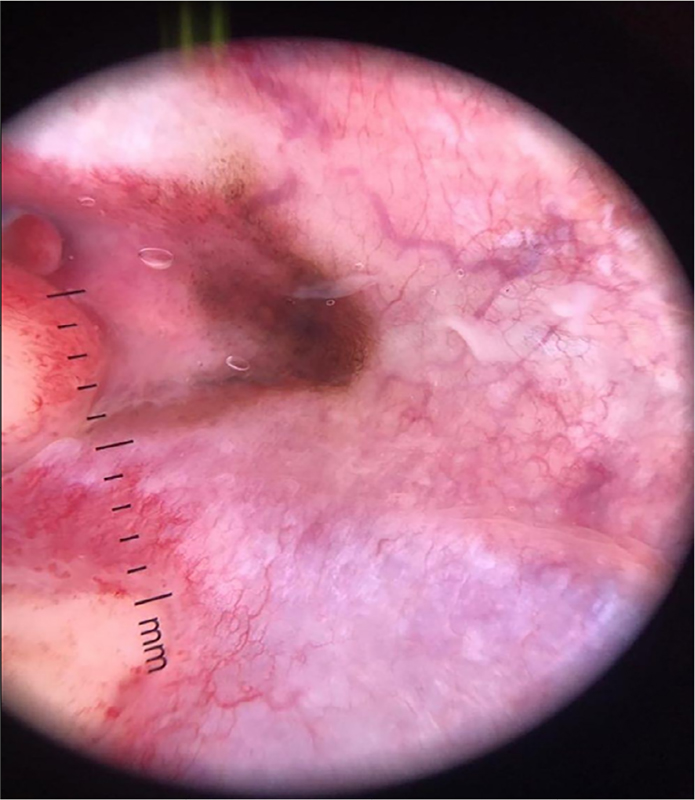
The patient underwent dermoscopy, a method for visualizing the structures located below the stratum corneum, being characterized as a hyperpigmented melanocytic lesion (Figure 2).
Figure 2 Dermoscopy (10x magnification): presence of atypical pigmented network with irregularly distributed spots, pigmented areas without structure (blotch), regression area, and bluish gray veil. Due to the suspicion of malignancy, an incisional biopsy of the lesion was performed.
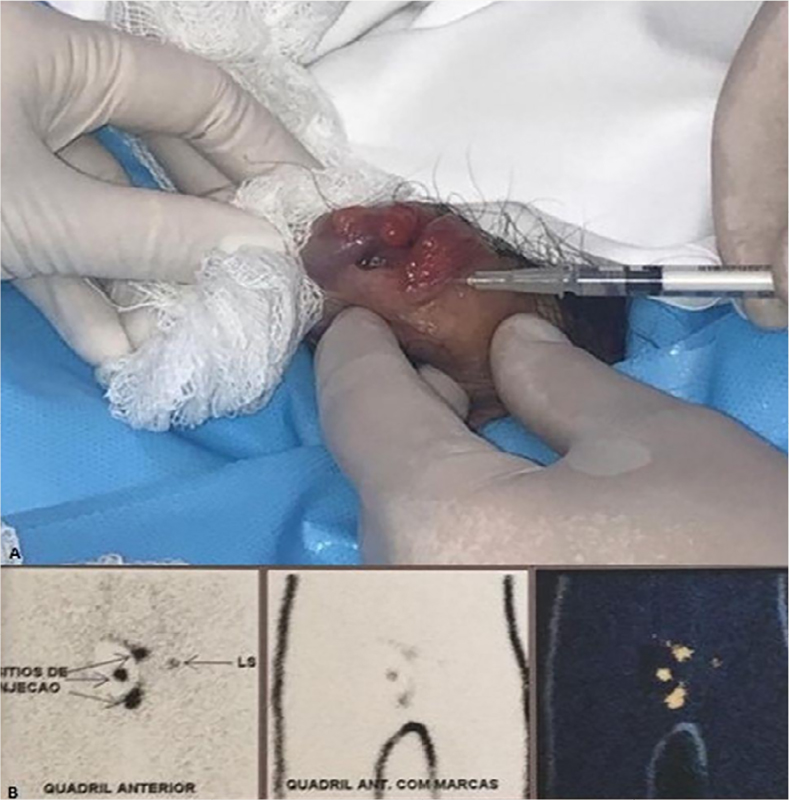
The anatomopathological showed a 7mm thick Clark IV nodular melanoma, with ulceration, without angiolymphatic and perineural invasion. Clinical staging of the disease was performed with chest X-ray, abdominal and pelvis tomography (CT) and cranial magnetic resonance imaging (MRI), with no evidence of regional lymph node enlargement or systemic metastases. Due to the locally advanced clinical stage (T4bN0M0 – ulcerated lesion above 4mm), PET/CT was performed, whose uptake also did not show lymph node or systemic disease. The authors performed partial penectomy and investigation of sentinel lymph node with local technetium injection 12 hours before the procedure (Figure 3), in addition to bilateral inguinal lymphadenectomy at the same surgical time, due to the absence of clinical evidence in the literature that proves the total effectiveness of the sentinel lymph node in the identification of lymph node micrometastasis of penile melanoma, since the lymphatic drainage of the penis is crossed, as it is a midline organ. The margin was subsequently enlarged by 2cm due to impairment (Figure 4).
Figure 3 A. Technetium injection 12 hours before the surgical procedure in triangulated points, close to the primary lesion on the penis; B. Lymphoscintigraphy showed uptake of the radiopharmaceutical in the left inguinal lymph node chain.
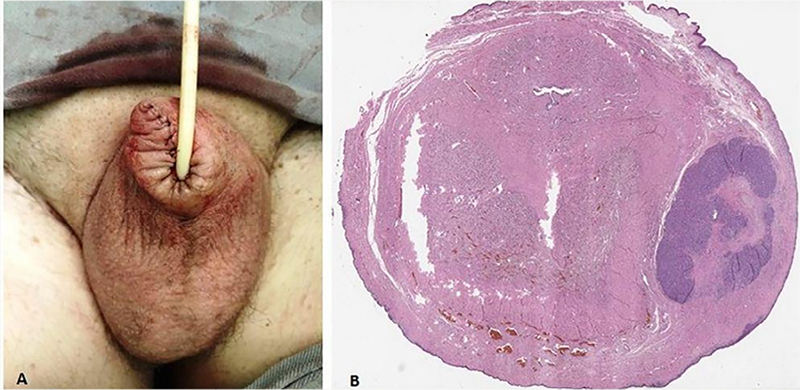
Figure 4 A. Post-operative result of penectomy and margin expansion; B. The anatomopathological study indicated vertical growth of the tumor, although there was an extensive lentiginous component “in situ”, associated with an area of ulcerated invasion with a thickness of 3.2mm that formed large groups of neoplastic melanocytes with atypical mitoses in the dermis and cavernous body.
There are microscopic satellite lesions that represent non-nodal regional tumor spread – pT3b pN1c pM0. The sentinel lymph node and the lymphadenectomy products showed reactive lymphoid hyperplasia, however the surgical margin was coincident with the lentiginous in situ component of the neoplasia. The surgical margin was then enlarged by 2cm, whose pathological and immunohistochemistry showed absence of neoplasia.
Primary penile melanoma (MPP) is a rare neoplasm that affects less than 1.4% of primary penile carcinomas and affects mainly patients in the sixth and seventh decade of life.[ 1 2 ] According to the histological origin of the tumor, penile melanomas can be divided into cutaneous and mucous. The cutaneous subtype is located on the penile shaft and corresponds to 9% of the locations. The mucous subtype is located in the glans (55%), foreskin (28%) and urethral meatus (8%).[ 1 4 ] One of the greatest challenges of MPP is its early diagnosis, since its initial presentation may be indistinguishable from benign injury. MPP can present as a black, brown, bluish, reddish or even amelanotic pigmented lesion.[ 5 6 ] Therefore, any suspicious lesion should be biopsied early.[ 5 ]
Several case reports describes the poor prognosis of primary penis melanoma, with 50% of patients already having some type of metastasis at the time of diagnosis.[ 10 ] The main factors of poor prognosis are: presence of ulceration, lymph node involvement, presence of microsatellite invasion, thickness greater than 3.5mm and diameter greater than 15mm.[ 5 ] The overall survival rate at 2 and 5 years is described at 63% and 31%, respectively.[ 5 ] The most accepted classification for melanoma follows the protocol established by the American Joint Committee on Cancer. Depth and the presence of ulceration are the most relevant factors in the TNM classification.[ 7 ] Between the 1970’s and 1980’s, treatment involved radical surgery (total penectomy, perineal urethrostomy and inguinal, iliac and bilateral obturator lymphadenectomy).[ 8 ] More recently, organ-sparing surgeries have become an option for individualizing treatment and consist of local excision, glandectomy, partial or total penectomy.[ 10 ] Treatment may involve the investigation of sentinel lymph node, a technique that detects the first lymph node chain affected by possible metastasis[ 8 ] and is an important in the prognosis of the disease, and that must be performed whenever there is a risk of hidden metastases.[ 9 ]
Other alternatives to melanomas that cannot be surgically excised include cryotherapy, radiotherapy and topical treatments such as interferons, azelaic acid, and fluorouracil, but evolve with a higher rate of recurrence. Imiquimod is an immunomodulator for the production of cytokines induced by the Toll-like receptor 7, used to treat actinic keratoses and basal cell carcinoma. Topical off-label use of imiquimod is reported in cases of melanoma in situ and metastasis of cutaneous melanoma, with an acceptable success rate.[ 11 ]
The prognosis for advanced disease is poor due to the low effectiveness of systemic chemotherapy.[ 4 ] Chemotherapy cycles are described with dacarbazine, carmustine, cisplatin and tamoxifen with an overall response rate of 45%.[ 4 ] The use of interferon reduces recurrence and increase the overall survival rate in advanced disease.[ 4 ] More recently, tyrosine kinase inhibitors and immunotherapy with checkpoint inhibitors (anti-CTLA4, anti-PD-1 and anti-PDL-1) have been used as adjuvant therapy after surgical resection to increase overall survival but due to the rarity of primary penis melanoma, there is no confirmation of safety and efficacy in this scenario.[ 7 ]
BRAF, a cytosolic protein kinase, whose activation leads to cell proliferation, was detected in melanomas outside the penis, enabling targeted therapy with some success. In a recent review, 12 patients with penile melanomas underwent DNA analysis, but none of these samples showed mutations in BRAF or activation mutations in exons 11, 13, 17 or 18 of the KIT. Reviewing the literature, we did not find evidence of BRAF mutation in a series of penile melanomas.[ 12 ] Primary radiotherapy (RT) can be considered in cases where resection is not possible, although most studies of RT involved few cases, short segment time and different doses of RT.[ 7 ]
Malignant melanoma of the penis is a rare disease whose incidence of metastasis is high due to the delay in diagnosis, and as a result, has low overall survival rates, even when it is treated. The gold standard treatment is resection of the lesion with organ-sparing surgery when possible. The investigation of sentinel lymph node and inguinal lymphadenectomy may be necessary depending on the stage of the lesion. The reported case shows a locally advanced penis melanoma whose treatment was partial penectomy, lymphadenectomy and margin enlargement, in an oncological follow up.
Journal: Brazilian Journal of Oncology
DOI: 10.1055/s-00059887
e-issn: 2526-8732
Publisher: Thieme Revinter Publicações Ltda.
Publisher address: Rua do Matoso 170, Rio de Janeiro, RJ, CEP 20270-135, Brazil
No references with the required fields found.